Raising awareness of mental wellbeing through Service Design
Organisation
IDC school of design
Industry
public health in developing countries
Year
jan 2021 - june 2021
Role
thesis project
Background
note
This project was a part of my Master's thesis at the IDC School of Design, under Dr Pramod Khambete and in collaboration with Tapas, an NGO for dementia care.
background & motivation
This project addresses a critical gap in the Indian mental healthcare landscape - awareness of mental wellness in middle-aged women (ages 40–55).
Despite being a population undergoing significant biological, psychological, and social transitions, these women remain underserved and often invisible in mental health discourse.
Cultural taboos, misattributed symptoms, religious coping mechanisms, and systemic invisibility often prevent timely intervention.
motivation
Motivated by personal observations and mentorship from professionals in the NGO and healthcare space, the project aims to create a service-oriented design intervention that fosters early awareness and proactive self-care.
Scope
scope
Since this is a complex, wicked problem, the project uses the Transtheoretical Model of Behaviour Change [1] focusing on the Pre-Contemplation and Contemplation stages - where awareness is either absent or just emerging.
Focus areas in the transtheoretical model of behaviour change

target groups
Two broad target groups were identified:
Priority Group: Middle-aged women (MAWs) themselves, to help them understand mental wellness, self-identify symptoms, engage in self-care routines, and access professional help when needed.
Influencing Group: Immediate family or community members, to build empathy, identify distress in women, and facilitate support.
Approach
The chosen approach was Service Design, enabling non-linear journeys and multi-stakeholder collaboration.
methods used
insights
Lack of mental health education
MAWs often defined wellness vaguely and misunderstood mental illness as a divine punishment or weakness.
Strong religious framing
Many women coped through faith rather than treatment, saying “God will take care of my problems.”
Neglect of self
Women prioritized family roles over self-identity, resulting in poor self-care and awareness.
Biological and social stressors
Menopause, empty nesting, caregiving responsibilities, and loneliness were common triggers.
Fear of being labeled
Seeking psychiatric help was perceived as shameful or 'crazy.'
Dependency on others
Many women only sought help if prompted by a trusted family member.
Secondary Research
methods used
insights from literature review
Cultural & Religious Framing
Explored how Islam, Hinduism, and Buddhism influence mental health narratives, e.g., illness as karma or imbalance.
Community Models in India
Highlighted successful grassroots interventions like Atmiyata Mitras [2] and peer support groups (e.g., AA model), as well as government initiatives like the Mental Healthcare Act, 2017.
insights from feature audit
An in-depth competitive analysis was done of seven mental health apps, including Woebot, Sanvello, Clementine, and Talklife.
Most apps were western-centric and did not resonate with Indian socio-cultural realities.
Features like journaling, CBT prompts, or motivational quotes were common, but lacked cultural adaptation.
This validated the need for interventions that were localized, community-supported, and emotionally resonant.
Ideation
Two stages of ideation
insights from literature review
First Round
Mapped ideas to the TTM stages and distinguished between interventions for individual women vs. their communities. Resulted in diverse but scattered ideas: WhatsApp forwards, Amar Chitra Katha-style comics, peer-led cooking workshops, and reflective quizzes.
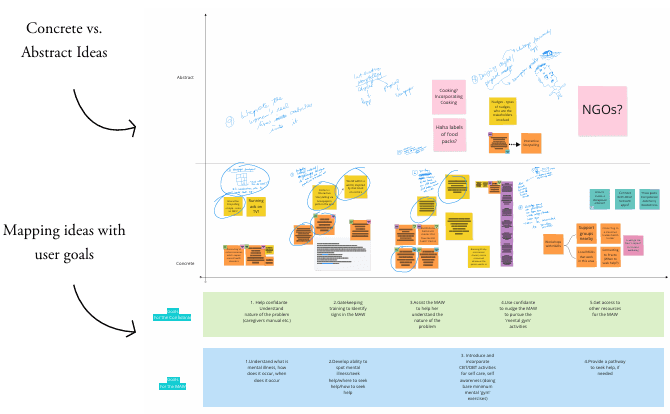
Second Round
Structured ideas by user goals (X-axis) and concreteness (Y-axis), creating a 2D matrix. This enabled the prioritization of actionable, high-impact ideas.
Ideation board: 01

Ideation board: 02
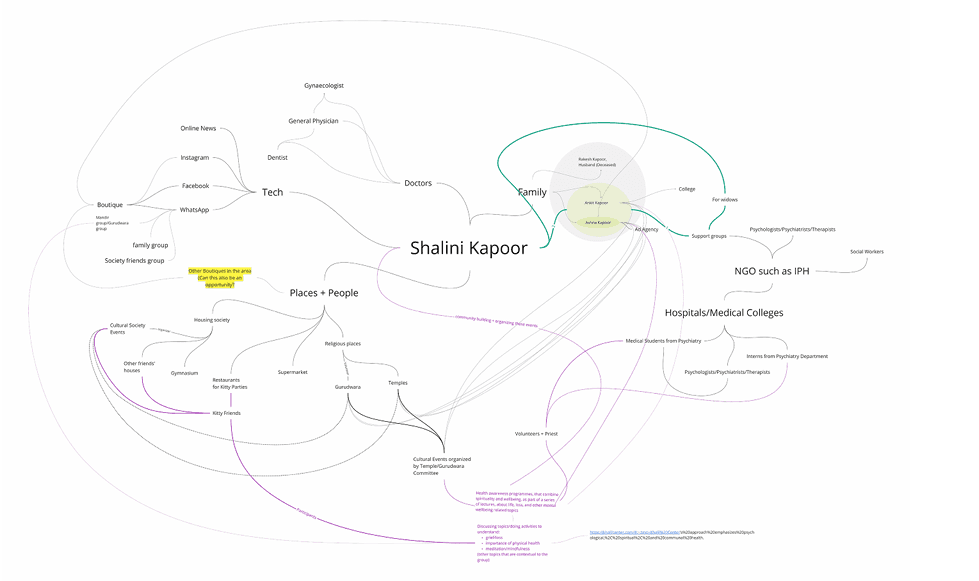
ecosystem maps
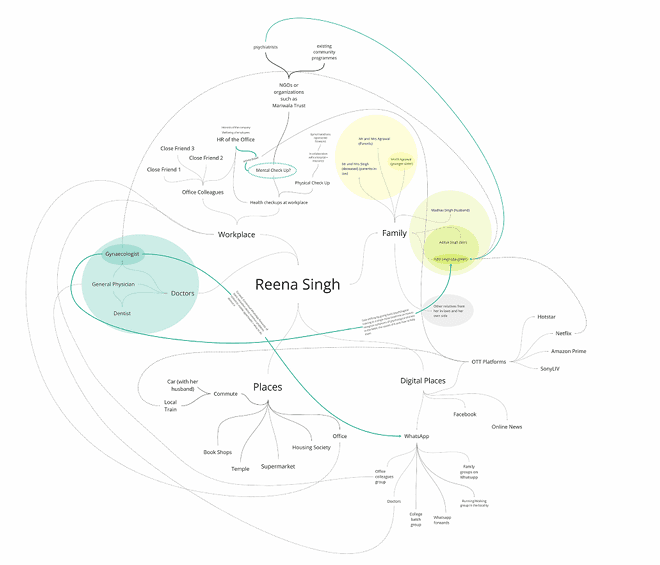
ecosystem maps
Final concepts
Concept 1
Bindaas Bol
An app integrating the best of three ideas—Mitran Programme (peer training), Duration-Based Activities, and Interest-Based Activities. Features included:
Mood-tracking stories based on Indian women’s lives
Reflective prompts and goal-setting nudges
Peer-moderated chat spaces
Onboarding flow adapted for tech-novice users

Concept 2
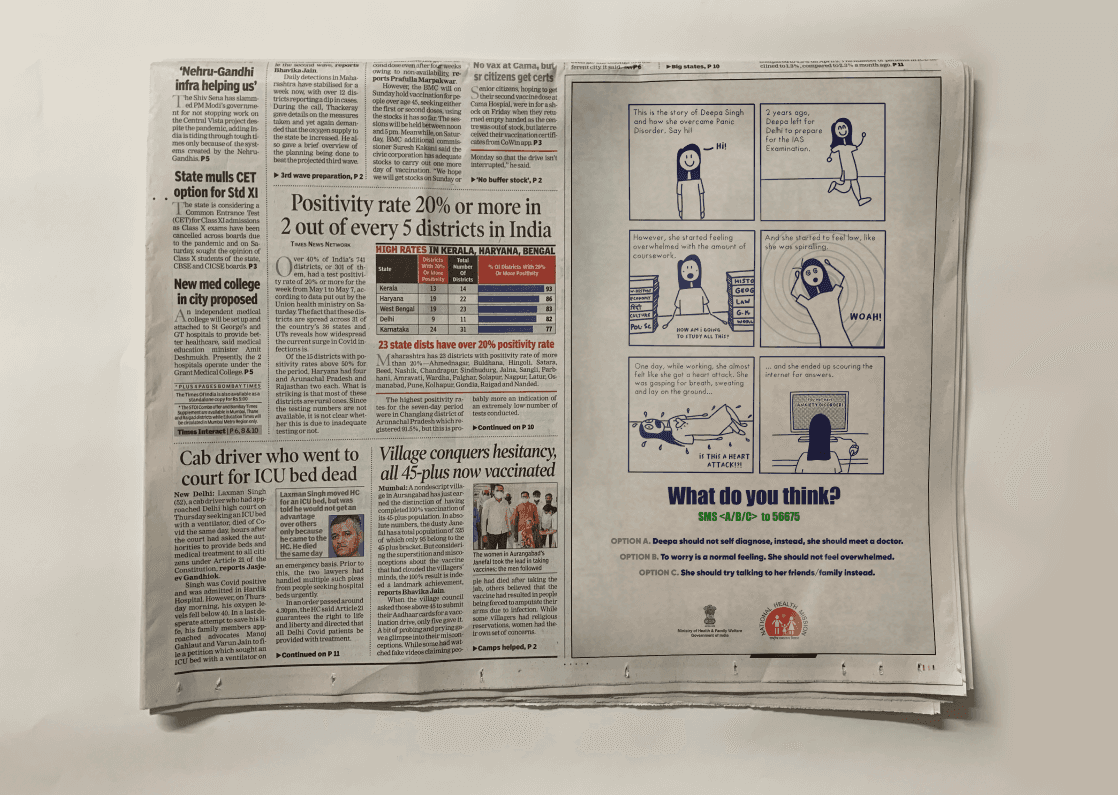
Interactive Comics
Short, narrative-driven comics based on real-life cases like Deepa’s story (panic disorder). Designed to be:
Visually simple (stick figures)
Emotionally relatable
Contextualized using familiar media like newspapers
Comics were tested both as physical prints and digital slides.
Concept 3
WhatsApp-Based Intervention
Daily nudges delivered via WhatsApp to simulate non-intrusive learning. Included:
Mental wellness tips
Links to short videos
Prompts to self-reflect
Effectiveness was mixed; engagement remained low, signaling that passive formats are insufficient for behavior change.

Evaluation
method used to evaluate
testing strategy
Each concept underwent small-scale testing with:
Three MAWs over 7–10 days (for WhatsApp-based simulation and talking through other concepts)
Four medical professionals via a Delphi-style feedback loop
key findings
Mitran Programme was rated most promising due to its systemic impact potential.
Bindaas Bol App was praised for simplicity and emotional nuance.
Comics were relatable, evoked empathy, and provided effective learning through story.
WhatsApp forwards, while appreciated, showed low interactivity and retention.
A common insight was the need for participatory, human-centered design—especially in a domain where shame and silence dominate.
learnings & reflections
This project underscored the emotional complexity of designing for taboo issues.
Behavioral change starts with attitude change. Creating space for reflection, not prescription, proved more effective.
Community and family inclusion are essential. Women often do not act on their own behalf; designing around social ecosystems proved key.
Subtlety matters. Using lighthearted storytelling and culturally rooted tools helped engage users without invoking defensiveness.
Frameworks like TTM help structure complexity in wicked problems.
The project emphasized how design can act not only as a problem-solving tool but as a bridge between silence and empathy.
References
[1] Prochaska JO, Velicer WF. The Transtheoretical Model of Health Behavior Change. American Journal of Health Promotion. 1997;12(1):38-48. doi:10.4278/0890-1171-12.1.38
[2] Joag K, Kalha J, Pandit D, Chatterjee S, Krishnamoorthy S, Shields-Zeeman L, Pathare S. Atmiyata, a community-led intervention to address common mental disorders: Study protocol for a stepped wedge cluster randomized controlled trial in rural Gujarat, India. Trials. 2020 Feb 21;21(1):212. doi: 10.1186/s13063-020-4133-6. PMID: 32085716; PMCID: PMC7035701.